Human gross anatomy is one of the first major rites of passage that medical students undergo on the way to becoming physicians. I won’t talk much about the emotional experience of it here, but let me just say that it is life changing and a true honor to experience. As you go through it, though, it can be easy to become desensitized to the emotion that is elicited by dissecting a human body, especially when there’s hundreds of structures to identify and ingrain in your memory. It is this sheer volume of information to learn that makes anatomy one of the hardest classes in the first year of medical school.
But I didn’t think it was that bad.
I did, however, have one advantage over many of my classmates – I had actually taught anatomy to undergrads (as a teaching assistant) and was currently teaching the class again as I went through my M1 anatomy course. I had learned alongside my undergraduate students as they studied the bones and their markings, muscles (their origins, insertions, actions, and innervations), and nerves – I had not taken anatomy before teaching it! While my knowledge of anatomy was not that great even after teaching (and was limited to those three systems), I did come away with a better understanding of how to effectively study for anatomy, and that made all the difference. Because of that, I would like to share some of my tips – both for medical students and my undergraduates – to help you all master anatomy!
Use the right resources
Your professor will likely assign a textbook for the class. We had Grey’s Anatomy for Students, which was helpful because it had an overview section in the beginning of each chapter that was a good place to start (and usually all that I read if I read the book at all). The book also has highlighted clinical correlations that were particularly good review for the written exam. It was also suggested (but not recommended) that we purchase an atlas, which I didn’t do until after the first semester (Netter’s Atlas of Human Anatomy is the shit). We had them available in lab, but it was incredibly helpful to have at home as well. While nothing can replace studying on actual cadavers (or models if your class also uses those), looking at images can be a good place to start/a good reference for clarification while/after looking at bodies/models/a good last minute review before the exam.
Another resource that is helpful is actually Wikipedia. While teachers 99.9% of the time tell you to never use Wikipedia (the information is unreliable, etc.), anatomy is the 0.1% of the time when it is an acceptable resource. My professor told us that anatomists have done a good job at maintaining the accuracy of these pages (though it is always important to cross check the information with your textbook/lecture notes, especially if your grading is strict like in the class I TA). Therefore, I mostly used Wikipedia for my information. I liked it because I could find out everything I needed (and then some) about a structure easily – I tend to learn things best by learning too much/putting it in greater context.
Make Connections
Nothing in the body exists in isolation. The most important part of anatomy is not just being able to identify individual structures but being able to understand their relations to each other. Learn to see how things are connected, whether through a direct interaction (this nerve innervates this muscle and thus runs along it) or indirect (this muscle lies next to this other muscle, and they are both innervated by the same nerve). By making these connections, you can reduce the number of pieces of information that you need to learn.
Spend time in lab wisely
The most important part of this first is that you NEED TO SPEND TIME IN LAB. I simply cannot emphasize that enough. I could definitely see a difference in scores between those students who came in extra times to lab to learn the material and those who did not. Anatomy is a highly visual and tactile subject. You need to see the muscles/arteries/nerves/etc. and understand where they are in relation to other structures. While Netter’s and other anatomy text books have pretty looking pictures, they cannot do the real human body justice. You need to look at both your body as well as other bodies in the lab since you’re likely going to be tested on all of them (see point #3 in my Almost Doc’s article 5 Precise Techniques to Become to Most Effective Learner Ever). No two bodies look exactly alike, and it is important to truly appreciate that.
You also need to spend your time in lab WISELY. My undergrad students are required to be in lab for 1.5 hours each class, most of that time being free time for them to learn from models/cadavers/etc. as they see best. But many of them would spend that time talking to friends (not about anatomy), working on things for other classes, sleeping, texting/facebooking/online shopping, or doing something else totally unrelated to class. Others would spend time superficially going through the bigger (and easier) items to learn, usually while looking up information online/in the text book. Very few would be actually using the models that they would be tested on (though they did spend a decent amount of time with the cadavers). Yet before every exam someone would ask for more time in lab to study. Had they come to lab with a plan and used their time to study things that they couldn’t study at home (such as looking at the models and cadavers that they would be tested on), they wouldn’t feel that they need any extra time.
The same idea of wisely using your time applies to M1 anatomy. Come to lab during the extra hours with an idea of what you want to study. My recommendation – start with the things you know the least. Everyone wants a confidence booster by going through the things they know the best, but that is low hanging fruit. To make the biggest leap in your understanding, you need to focus on increasing knowledge in areas that you understand the least (see the personalize section in my blog post Study Tips for the MCAT (More on How I Prepared in a Month)). For me this was usually arteries and nerves – they can be hard to differentiate, there’s lots of branching – so I would try to start with these areas that I knew the least and try to go through the whole structure list for those areas before moving on to topics that I was more comfortable with.
Have a study buddy
One of the best things that I did was study with other people. I was fortunate to be placed with a great dissection group of super intelligent human beings who were both fun and hard working – the perfect study buddies. We were thorough during our scheduled dissection times (usually using the whole time if not going longer) and often some of us would meet up at other times to go over our dissections. I’m not one to study with other people, but in anatomy this was essential.

The benefits of studying with others are many. First of all, they can help you flip a body if need be (something I tried to avoid at all costs). Second, they probably know things that you don’t know and vice versa. We would usually go through our structure list and take turns teaching each other/quizzing each other. By reading a term, saying it out loud, identifying it on a body, and having confirmation from another person, you are giving yourself more opportunities to have that information ingrained in your memory. Also, not knowing a term, being quizzed on it, and having someone explain it helps you learn from being wrong/not knowing. Of course, working together to figure out something neither of you know is also quite helpful (make sure to have text books/atlases available to reference while in lab).
Perhaps one of my favorite benefits of studying with others is learning how they remembered a structure. We all hear different mnemonics that can help us learn. Sometimes it’s not a mnemonic but rather an interesting connection/observation that stands out to remember a term. One of my favorite examples of this is the transverse cervical artery that runs vertically just deep to the trapezius muscle. When the trapezius muscle is dissected, it can be flipped to the side to see underlying structures, including the artery. Thus the artery, which goes with the muscle, appears to be running in the transverse plane of the body. One of my lab mates excitedly pointed this out, and even though the artery doesn’t run in the transverse plane when placed in anatomical position, I always remembered the name of the artery that lies under the trapezius because of this discussion.
Make your own study guides
I’m a big fan of making my own study guides. I do this not only for anatomy but many of my other classes as well. Everyone learns information a little differently and by making your own study guide, you can display this information in the way that makes the best sense for you to remember it. Also, simply the act of writing things down is helpful for memorization (which is why I HIGHLY RECOMMEND doing this especially for learning the CORRECT SPELLING of these terms, which is often a component of your grade). For anatomy, I would go through my whole structure list and make study guides based on the topic for all of the structures. By doing so, I learned a couple of very useful techniques to make the most effective study guides that I describe below.
Use tables
I never appreciated tables until I took anatomy. As an example of how I used tables, see the image below:
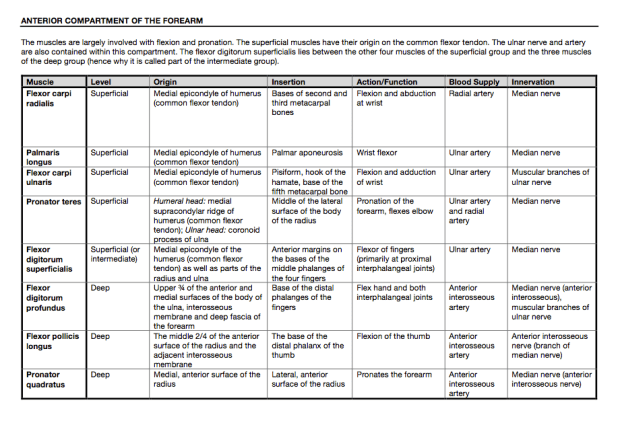
This is the table I used to learn the muscles in the anterior compartment of the forearm (a connection between these 8 muscles). For most of my muscle tables, I only included the origin, insertion, action/function, blood supply, and innervation. However, I also included level (superficial vs. deep) to understand the relative location of these muscles since there are so many in this compartment (and I listed them superficial to deep). Having all of this information in a table is helpful to see the connections between structures. For example, you can see that the three muscles listed as being “deep” are also supplied by the anterior interosseous artery while those being “superficial” are supplied by the ulnar artery. This also hints at the location of these arteries. You can also see that the three superficial wrist flexors all have their origin at the medial epicondyle of the humerus.

I also made tables for other topics such as nerves that I didn’t necessarily need to have multiple columns like for muscles. However, I made the table as a replacement for writing out notecards (since writing that much would take forever and would destroy my hand). Though writing by hand has been shown to be better than typing for retention, I tried to do things like emphasizing parts my writing (see the bolded words to emphasize a connection to another term, other times I used all capital letters, italics, or underlines to emphasize different things). By having changes in formatting, I was able to have important parts of what I wrote come across easier.
Make a list
One of the biggest revelations I made when making study guides was how to learn the branching pattern of nerves and arteries. Initially, I would make a table for these (like I did for muscles) that included source and branches. But then I figured out to make things like this:

This may just look like a list to you, but it is actually a very well thought out list that gives away much more than just the structure names. The terms are listed in order of how they are found – proximal to distal. Each indentation indicates that the artery is a branch of the artery above it. For example, if you wanted to know how the common interosseous artery in the forearm arose, you would be able to see that it is a branch of the ulnar artery, which is a branch of the brachial artery, which is a branch (well actually a continuation) of the axillary artery. You can also see that the common interosseous artery comes off of the ulnar artery after the posterior ulnar recurrent artery and before the anterior interosseous artery. I would bring these lists in lab to go through as I tried to identify all of these terms on the body. A major benefit is that it is concise (and usually fits on a single page) but provides a lot of information!