
With the elderly proportion of the US population growing, bladder cancer may become more widespread in a population that is not well understood.

I could barely recognize my grandmother’s frail body as she lay on a hospital bed in the room that was once her dining room. She asked what the weather was like outside. Fighting back tears, I told her it was a nice sunny day and there were robins on the bird feeders that she liked to watch on her deck. It was comforting to see her face light up at the thought, but I knew it was really a gloomy April day with no birds in sight.
I did everything that I could to not think of the tumor growing in her bladder that day, but like a tumor in my mind, the realization that this was her end was growing into an overwhelming force. Each time she exhaled, there would be a long pause where I would stroke her hand fearing she would never breathe again. Her sister told her what I did not have the strength to: “You are dying.” The family knew since her diagnosis that this day was coming soon.
—
It all began the previous August when my grandmother, a relatively healthy woman of 85, saw her doctor because she was experiencing painful urination and blood in her urine. These symptoms pointed toward a urinary tract infection (UTI), a condition that over half of women will get at least once in their lives. With a history of UTIs, she was given antibiotics and sent on her way.
The relief was short-lived. In September, the symptoms returned and she went back to the doctor. At her age with antibiotic treatment unable to completely dismiss the symptoms of a UTI, he knew something was up. She was referred to a urologist who used a camera to look insider her bladder, a technique known as a cystoscopy. This confirmed the family’s greatest fear – it was cancer.
Her age put her at higher risk for bladder cancer. Adjusting for population size, twice as many over 85 are diagnosed with bladder cancer than those in their 60s. Their cancers are also often at a more advanced stage, being over four times more likely to develop invasive bladder cancer. With the proportion of elderly in the US expected to double by 2030, the prominence of bladder cancer, especially more aggressive and invasive bladder cancer, will likely rise as the proportion of elderly increases. What’s worse is that unlike their younger counterparts, the elderly are less likely to receive thorough treatment of the disease and are more likely to die from it.
Considering her age, her oncologist gave her the option of extending her life with chemotherapy or relieving her symptoms with a surgery that could cut out as much of the tumor as possible. While chemotherapy would possibly come with complications such as high fevers and discomfort that are more problematic in the elderly, the surgery would be only palliative and so the tumor would likely grow again. Not wanting to extend her suffering, she opted for the surgery leaving her lifespan up to the growth of abnormal cells in her bladder.
Bladder cancer in the elderly is not well studied. While assumptions can be made from what is known about its effects on younger populations, the physical, mental, and social changes that occur with aging may lead to different disease outcomes. Because of this ambiguity, we were unsure whether my grandmother had a matter of years, months, weeks, or even days left with us.
To ease our worries about how long my grandmother had to live, her oncologist told her to have a scan in 3 months to check the cancer’s progression. Since it’s especially difficult to predict lifespan in elderly with the disease, this at least gave us a goal. For her, a more important goal was getting to Christmas when my cousin would be visiting from California and bringing her newborn son for my grandmother to meet for the first time.
For women, the prognosis of bladder cancer is less hopeful than for men as they are more likely to die in the first 3-4 years after diagnosis. Like my grandmother, they’re more likely to receive symptomatic treatment for a UTI within a year before being diagnosed with bladder cancer. This delay in diagnosis along with other prognostic variables such as age and tumor stage still only explains 30% of the excess mortality compared to men. The other 70% may be attributed to hormonal differences and other factors.
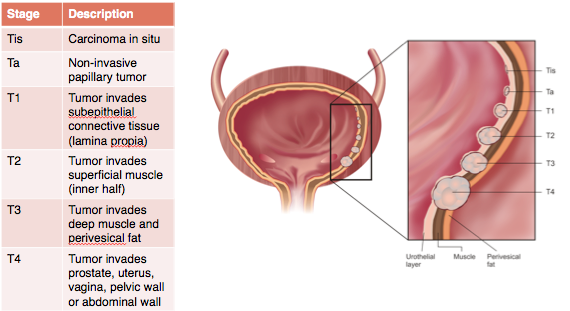
By the time my grandmother’s tumor was found it had reached the most advanced stage of cancer. It had invaded the epithelial layer of cells lining the bladder and had gone into the muscle. Her lymph nodes were also enlarged and her oncologist suspected that the cancer had spread there as well. I later learned that she could have been offered a radical cystectomy, a surgery where the bladder is removed and replaced with a piece of intestine that functions to hold urine like the bladder. This surgery is the gold standard for muscle-invasive bladder cancer.
Analysis of the SEER database, a government collection of surveillance, epidemiology, and end results regarding cancer, shows that of those patients with cancers needing this more invasive surgery, 55% of those aged 55-59 had the surgery while only 25% of those aged 70-79 did. Shahrokh Shariat, a distinguished professor of urology at Weill Cornell Medical College, hypothesized that this disparity may be due to the overuse of non-surgical alternatives, the inexperience of surgeons, or what was likely my grandmother’s case, the potential belief that older patients may not be able to tolerate the surgery.

Caring for her family has always played a large role in my grandmother’s life. After marrying my grandfather at 21, she raised three daughters who gave her seven grandchildren and three great-grandchildren. She supported us in our childhoods by teaching us piano, playing tennis with us late into her 70s, and doing everything else that she could to be involved in our lives. As her grandchildren grew up and needed less of her attention, she was then more capable of caring for my aging grandfather.
With her diagnosis, she went from caregiver for her 89-year-old husband to being needed to be cared for as well. She not only had to prepare his meals, take him to doctor appointments, and watch out for him falling, but she had to worry about her own health issues. The family that she helped raise stepped in to take some of the weight off of her shoulders, but we could only do so much to mitigate the strain of her disease on her mind and body.
Christmas soon arrived and she was able to hold her great-grandson in her arms for the first time. The most wonderful time of the year also meant that she had made it to the three-month mark and needed to have a scan to see how the cancer had progressed. After much anticipation, the results were in. “It grew,” her oncologist said, “But not as much as expected.” Any bit of positive news was good enough for us to celebrate.

This joy was only temporary. Early in February, she again saw blood in her urine that became heavier as the day passed. While she hoped it would go away, it did not. My aunt came to stay with her in case the blood loss affected her. They decided to call 911 and she was rushed to the hospital where she was tested for kidney function and bladder infection, but the tests came back fine meaning that her cancer was likely the culprit.
Her urologist suggested that she could try to repeat the surgery she had in the fall to alleviate these symptoms, and the next Friday she went in for late afternoon surgery. As it was minimally invasive, she was sent home later that evening without the nurses even checking if she could urinate. She couldn’t. My aunt brought her to the emergency room that night for a catheter, upset by the huge inconvenience brought upon them both.
Again, the relief was short lived. While the first surgery brought months of minimal symptoms of her disease, they returned just weeks after her second surgery. A difficult discussion with her doctor came to the conclusion that it was time for her to go on hospice, at-home palliative care. She would then be able to spend the rest of her life in the comfort of her own home with nurses visiting the house and medications coming by delivery.

While my grandmother’s health had been declining before, on hospice, it was plummeting. The pain she felt was not want she anticipated when opting to not do chemotherapy, and part of her regretted the choice. We reminded her of the complications associated with chemotherapy, which reassured her that she made the best decision considering her circumstances.
Concerned that her days were numbered, her sister flew in from Seattle to stay with her for the duration. An aunt from San Diego took the first flight she could, intending on being in Minnesota with the family as much as her job allowed. The cousin from California also came for a few days with her sons. “Everyone’s coming to visit me,” my grandmother said. “Am I dying?”
Over the month and a half she was on hospice, I watched my grandmother slowly succumb to the growth that manifested in her bladder. Her skin appeared paler and her energy level dropped. I’d often see her trying to do what she would have done normally – crossword puzzles, knitting, reading books – but really she’d just be staring off, lost in her own thoughts. She became confused, not remembering what happened which day or who said what. Her pain medications sedated her and she’d go in and out of consciousness mid-conversation.
Even more, she began feeling nauseous more often and went on anti-nausea medication. Its side effects were almost worse than the nausea itself. The foods that she once loved were no longer appealing to her. By Easter, she could barely keep anything down and watched us all eat our dinners while she struggled with some ice chips.
The human body has enough stored energy to go several weeks without food, but without fluids, a person has a matter of days left. On the morning of April 6, my grandmother tried to drink water but instead of it going to her stomach, it went into her lungs. The hospice nurse said to no longer give her water. It was her time to go.
I got to the house as soon as I could. My mother brought me to the dining room and I sat next to my grandmother’s hospital bed. Though there had been seven months since her diagnosis to prepare for this day, I couldn’t find the right words. Instead, I spoke with her about the weather and birds, anything simple that she’d know and love, and told her she looked beautiful. She’d ask for water, but all we could do is wet her mouth with a washcloth. In her frequent moments of confusion, she’d begin worrying about various things, but we didn’t know what she meant by her slurred words. “Don’t worry,” my mother said, “Today is just a day for you to relax.”
To not overwhelm my grandmother and give the rest of the family time to see her, I eventually said my goodbye and left. I waited the whole day for word that her suffering was over, longing for her to be at rest. Still she persisted through the afternoon and into the evening. At 10:24 p.m., a wave of relief swept over me as I read my mother’s text that said, “Grandma is at peace now!” Finally, we were all at peace.

{kind=link}