Q (from ask.fm): As a MD/PhD student, do you have any time for yourself? For family and friends? To just take a break? I would like to do a MD/PhD program, but I want to enjoy my 20s…
A: Of course you have time! I fully want to enjoy my 20’s as well so even if I don’t feel like I have time, I MAKE time to enjoy it. When you’re in the graduate portion of your PhD, your free time is really based on how much your PI will push you (or how much you push yourself). It is an important consideration when you pick a lab. If the PI is understanding and aware that people are not robots who just work 24 hours a day to produce data, then you should be granted the time that you need. In fact, I’ve had PI’s tell me to go home because I’m in lab too late or I’m there on a weekend!
I actually just read a blog post today about this culture of pushing scientists too far (in response to a sad situation), and a particular quote from it stood out to me:
“The best (and more importantly, happiest) scientists I know are people who are interested in many things, who approach all aspects of their lives with engagement, purpose and openness.”
There seems to be a cultural shift away from pushing students too hard, which makes me glad. Obviously, we want to be successful and have a lot expected of us (which only increases as we progress through our careers), but we have to appreciate our own limits as well.
As someone who enjoys writing for fun, watching sports games, enjoying my weekend nights out with friends, going home to see family and friends (which requires an eight hour drive one way for me right now), playing musical instruments, and many more leisurely activities, I believe that doing so makes me better at what I do by keeping me happy and healthy. I believe that everyone can make time to have a life if they work hard enough to do so. Not only that, I also believe that they all SHOULD. It may take a little work to figure out how to balance everything, but it can be done and it is definitely worth it. As long as you find a program and an advisor that understands that you need to have a life outside of school, you will have the time that you need.
When I began thinking about writing, I had a dream that I could someday reach out to the world and educate them with my writing. I wanted to be like Siddhartha Mukherjee, the author of one of my favorite books, The Emperor of All Maladies: A Biography of Cancer, who is both an oncologist and an award-winning science writer.
Alas, the task to reach out to others, create an entertaining, informative, and educating piece of work seemed to me to be a formidable task. But then again, the science writers I looked up to wrote entire books – books that took years and years for them to write. Clearly, my goals were set high. I took a step back, breathed, and realized I had to start somewhere smaller, so I signed up for a class called “Writing on Issues of Science and Technology.”
The description of this class said the instructors would choose topics that can include:
DNA and the Human Genome (Good start!)
Animal/Human Cloning and Stem-Cell Research (Right up my alley)
Vaccines from Smallpox to AID (Could there be a better fit?)
Global Warming (Not my area of focus, but I still find it interesting)
Alternative Energies (I could probably deal)
Animal/Human Interaction (Not as much my thing)
Why Civilizations Collapse (I don’t even know…)
I took my chances. About half of the topics were exactly what I’d hope to write on (those most related to medical sciences) and half were not. Turns out, my professor picked exactly what I didn’t want to write about. When I looked at the book list for the course, half of them were about studying wolves in nature and the other half gorillas. Not only were we not focusing on topics I wanted to write about, we were barely even writing. Instead, we were reading science writing books. Nonetheless, I bought the books and started going to the classes.
My professor was a cute old woman with a soft voice and long graying hair who loved to get side tracked and tell us stories about her day. At first, I was frustrated with her taking away discussion time, but I grew to love her stories. In one of these stories, prior to beginning discussion on the first book we were reading, she mentioned she was teaching another class, “Science Writing for Popular Audiences.” BINGO. I found my class.
Though I didn’t have the writing course prerequisite, I explained to her my desire to actually write and my background in science that compelled me to do so. Without hesitation, she let me switch courses. Just a few weeks into the semester, I found myself walking into my first Science Writing for Popular Audiences class and surprise, surprise, our first topic to write about was the wolves of Isle Royale.
Clearly, this professor had a liking towards wolves.
This time, though, instead of reading about the wolves, I had the chance to write about them. Our prompt was to research the wolves and write an article that would explain to the reader the current dilemma the wolves on this island faces.
If you don’t know, Isle Royale is a small island in Lake Superior, just 20 miles from the mainland. It is inhabited with moose, loaded with fir trees, and in 1949, two grey wolves crossed an ice bridge from the mainland and started a wolf population on the island. It is also home to the longest running closed system predator-prey study. If you’ve ever learned about population dynamics (you may have to think back a ways – I can recall making mathematical equations to represent it in my high school math classes), the data for the basis for understanding the fluctuation of predator and prey likely came from this island.
Over the more than 50 years of this study, the wolf population has fluctuated along with the moose, reaching a maximum of 50 in the late ‘70s. This fluctuation was thrown off soon after that peak as a virus killed of many of the wolves. Ever since, the pattern of rise and fall no longer fit our expectation from the first half of the study and today, the wolf population is the lowest since the study began.
What seemed like a simple task – write about the wolf population – was much more difficult than I could have ever imagined. I had so much that I wanted to write about this island, rich in history, and the shrinking wolf population that there was no way I could fit it all into 750 words.
My first edition of my paper, to say the least, was atrocious. Used to writing reports and simply telling like it is, I was not the greatest at turning information into a story. Luckily, my professor gave me a second shot.
I took a step back and looked at my paper, cutting nearly all of it. No, I didn’t need to spend half of it talking about the history of the study, the fluctuation of the wolves; I needed to talk about here and now. I also decided to take a different angle, to give an overall story of the situation the wolves are facing, not the issue the researchers are facing looking at the wolves. After much rewriting, I ultimately came up with a piece I was proud to call mine, Isle Royale’s Drama of Survival.
Most importantly, during this process, I went from hating that I had to write about wolves, to loving these wolves.
Living close to Lake Superior, I wanted to take a trip to the National Park on the island to see where the wolves live. I obsessively kept track of the researcher’s blog as they did their winter survey. I was scared every time I checked it to see if Isabelle, a lone wolf on the island and one of the only remaining females, had been killed by the pack that was pursuing her. When the study of 2013 was done and updates were no longer given, I continued to think of Isabelle.
Isabelle cornered following an attack.
I was excited to hear that she was seen again on the island this winter. The researchers last saw her on January 21st, heading toward her assailants. There have been a few ice bridges formed to the mainland this year, the kind of bridges that brought wolves to the island, but that can also let them leave. The researchers believe she left the island via ice bridge that night.
She made it… her carcass was found on the mainland on February 8.
Today, I mourn the loss of Isabelle but also have hope for the island. Three pups were born this year, the first pups for some time. Yet, the issue of inbreeding remains and the debate to intervene continues. Nonetheless, I’m glad I stuck with this class despite lack of appeal a wolf study originally had to my medically-oriented self. I learned to become a better writer, wrote my first science writing piece, and I was introduced to these wolves who will always have a special place in my heart.
I could barely recognize my grandmother’s frail body as she lay on a hospital bed in the room that was once her dining room. She asked what the weather was like outside. Fighting back tears, I told her it was a nice sunny day and there were robins on the bird feeders that she liked to watch on her deck. It was comforting to see her face light up at the thought, but I knew it was really a gloomy April day with no birds in sight.
I did everything that I could to not think of the tumor growing in her bladder that day, but like a tumor in my mind, the realization that this was her end was growing into an overwhelming force. Each time she exhaled, there would be a long pause where I would stroke her hand fearing she would never breathe again. Her sister told her what I did not have the strength to: “You are dying.” The family knew since her diagnosis that this day was coming soon.
—
It all began the previous August when my grandmother, a relatively healthy woman of 85, saw her doctor because she was experiencing painful urination and blood in her urine. These symptoms pointed toward a urinary tract infection (UTI), a condition that over half of women will get at least once in their lives. With a history of UTIs, she was given antibiotics and sent on her way.
The relief was short-lived. In September, the symptoms returned and she went back to the doctor. At her age with antibiotic treatment unable to completely dismiss the symptoms of a UTI, he knew something was up. She was referred to a urologist who used a camera to look insider her bladder, a technique known as a cystoscopy. This confirmed the family’s greatest fear – it was cancer.
Her age put her at higher risk for bladder cancer. Adjusting for population size, twice as many over 85 are diagnosed with bladder cancer than those in their 60s. Their cancers are also often at a more advanced stage, being over four times more likely to develop invasive bladder cancer. With the proportion of elderly in the US expected to double by 2030, the prominence of bladder cancer, especially more aggressive and invasive bladder cancer, will likely rise as the proportion of elderly increases. What’s worse is that unlike their younger counterparts, the elderly are less likely to receive thorough treatment of the disease and are more likely to die from it.
Considering her age, her oncologist gave her the option of extending her life with chemotherapy or relieving her symptoms with a surgery that could cut out as much of the tumor as possible. While chemotherapy would possibly come with complications such as high fevers and discomfort that are more problematic in the elderly, the surgery would be only palliative and so the tumor would likely grow again. Not wanting to extend her suffering, she opted for the surgery leaving her lifespan up to the growth of abnormal cells in her bladder.
Bladder cancer in the elderly is not well studied. While assumptions can be made from what is known about its effects on younger populations, the physical, mental, and social changes that occur with aging may lead to different disease outcomes. Because of this ambiguity, we were unsure whether my grandmother had a matter of years, months, weeks, or even days left with us.
To ease our worries about how long my grandmother had to live, her oncologist told her to have a scan in 3 months to check the cancer’s progression. Since it’s especially difficult to predict lifespan in elderly with the disease, this at least gave us a goal. For her, a more important goal was getting to Christmas when my cousin would be visiting from California and bringing her newborn son for my grandmother to meet for the first time.
For women, the prognosis of bladder cancer is less hopeful than for men as they are more likely to die in the first 3-4 years after diagnosis. Like my grandmother, they’re more likely to receive symptomatic treatment for a UTI within a year before being diagnosed with bladder cancer. This delay in diagnosis along with other prognostic variables such as age and tumor stage still only explains 30% of the excess mortality compared to men. The other 70% may be attributed to hormonal differences and other factors.
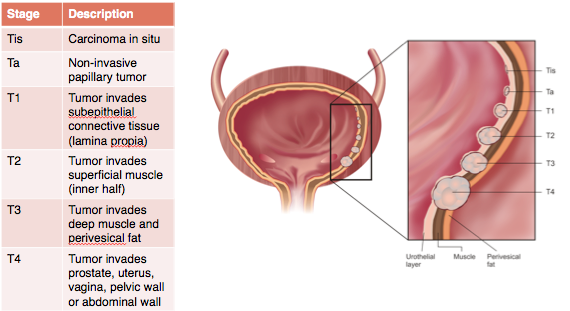
By the time my grandmother’s tumor was found it had reached the most advanced stage of cancer. It had invaded the epithelial layer of cells lining the bladder and had gone into the muscle. Her lymph nodes were also enlarged and her oncologist suspected that the cancer had spread there as well. I later learned that she could have been offered a radical cystectomy, a surgery where the bladder is removed and replaced with a piece of intestine that functions to hold urine like the bladder. This surgery is the gold standard for muscle-invasive bladder cancer.
Analysis of the SEER database, a government collection of surveillance, epidemiology, and end results regarding cancer, shows that of those patients with cancers needing this more invasive surgery, 55% of those aged 55-59 had the surgery while only 25% of those aged 70-79 did. Shahrokh Shariat, a distinguished professor of urology at Weill Cornell Medical College, hypothesized that this disparity may be due to the overuse of non-surgical alternatives, the inexperience of surgeons, or what was likely my grandmother’s case, the potential belief that older patients may not be able to tolerate the surgery.
My grandparents’ wedding photo (1948)
Caring for her family has always played a large role in my grandmother’s life. After marrying my grandfather at 21, she raised three daughters who gave her seven grandchildren and three great-grandchildren. She supported us in our childhoods by teaching us piano, playing tennis with us late into her 70s, and doing everything else that she could to be involved in our lives. As her grandchildren grew up and needed less of her attention, she was then more capable of caring for my aging grandfather.
With her diagnosis, she went from caregiver for her 89-year-old husband to being needed to be cared for as well. She not only had to prepare his meals, take him to doctor appointments, and watch out for him falling, but she had to worry about her own health issues. The family that she helped raise stepped in to take some of the weight off of her shoulders, but we could only do so much to mitigate the strain of her disease on her mind and body.
Christmas soon arrived and she was able to hold her great-grandson in her arms for the first time. The most wonderful time of the year also meant that she had made it to the three-month mark and needed to have a scan to see how the cancer had progressed. After much anticipation, the results were in. “It grew,” her oncologist said, “But not as much as expected.” Any bit of positive news was good enough for us to celebrate.
My grandmother holding her great-grandson (2013)
This joy was only temporary. Early in February, she again saw blood in her urine that became heavier as the day passed. While she hoped it would go away, it did not. My aunt came to stay with her in case the blood loss affected her. They decided to call 911 and she was rushed to the hospital where she was tested for kidney function and bladder infection, but the tests came back fine meaning that her cancer was likely the culprit.
Her urologist suggested that she could try to repeat the surgery she had in the fall to alleviate these symptoms, and the next Friday she went in for late afternoon surgery. As it was minimally invasive, she was sent home later that evening without the nurses even checking if she could urinate. She couldn’t. My aunt brought her to the emergency room that night for a catheter, upset by the huge inconvenience brought upon them both.
Again, the relief was short lived. While the first surgery brought months of minimal symptoms of her disease, they returned just weeks after her second surgery. A difficult discussion with her doctor came to the conclusion that it was time for her to go on hospice, at-home palliative care. She would then be able to spend the rest of her life in the comfort of her own home with nurses visiting the house and medications coming by delivery.
The house where my grandmother spent her last days
While my grandmother’s health had been declining before, on hospice, it was plummeting. The pain she felt was not want she anticipated when opting to not do chemotherapy, and part of her regretted the choice. We reminded her of the complications associated with chemotherapy, which reassured her that she made the best decision considering her circumstances.
Concerned that her days were numbered, her sister flew in from Seattle to stay with her for the duration. An aunt from San Diego took the first flight she could, intending on being in Minnesota with the family as much as her job allowed. The cousin from California also came for a few days with her sons. “Everyone’s coming to visit me,” my grandmother said. “Am I dying?”
Over the month and a half she was on hospice, I watched my grandmother slowly succumb to the growth that manifested in her bladder. Her skin appeared paler and her energy level dropped. I’d often see her trying to do what she would have done normally – crossword puzzles, knitting, reading books – but really she’d just be staring off, lost in her own thoughts. She became confused, not remembering what happened which day or who said what. Her pain medications sedated her and she’d go in and out of consciousness mid-conversation.
Even more, she began feeling nauseous more often and went on anti-nausea medication. Its side effects were almost worse than the nausea itself. The foods that she once loved were no longer appealing to her. By Easter, she could barely keep anything down and watched us all eat our dinners while she struggled with some ice chips.
The human body has enough stored energy to go several weeks without food, but without fluids, a person has a matter of days left. On the morning of April 6, my grandmother tried to drink water but instead of it going to her stomach, it went into her lungs. The hospice nurse said to no longer give her water. It was her time to go.
I got to the house as soon as I could. My mother brought me to the dining room and I sat next to my grandmother’s hospital bed. Though there had been seven months since her diagnosis to prepare for this day, I couldn’t find the right words. Instead, I spoke with her about the weather and birds, anything simple that she’d know and love, and told her she looked beautiful. She’d ask for water, but all we could do is wet her mouth with a washcloth. In her frequent moments of confusion, she’d begin worrying about various things, but we didn’t know what she meant by her slurred words. “Don’t worry,” my mother said, “Today is just a day for you to relax.”
To not overwhelm my grandmother and give the rest of the family time to see her, I eventually said my goodbye and left. I waited the whole day for word that her suffering was over, longing for her to be at rest. Still she persisted through the afternoon and into the evening. At 10:24 p.m., a wave of relief swept over me as I read my mother’s text that said, “Grandma is at peace now!” Finally, we were all at peace.
Surviving as a lone wolf is difficult, but for Isabelle, the winter of 2013 posed a greater challenge. Targeted by another female and her two companions, her life was in danger as they attacked with the intensity used to take down a full size moose, jaws clenching hard aiming to rip muscle from bone. Had these wolves known that Isabelle, a close relative to every male wolf on the island, had low reproduction potential, perhaps they would have realized that she was not a threat. But for her female assailant, she was seen as breeding competition to eliminate.
Wolves have inhabited Isle Royale since 1949 when a pair crossed an ice bridge spanning the 20 miles of Lake Superior separating the island from the mainland. Their numbers rose until 1980 when their population size plummeted from 50, the all-time high, to 14 in just two years after evidence of a deadly canine parovirus was first seen in the blood of the animals. This population crash drastically shifted the wolves’ population dynamics. Before the crash, wolf numbers fluctuated based primarily on the number of older moose on the island, but after, there was little correlation. Instead, the genetic effects of their isolation took hold.
With a limited gene pool, wolves have become more inbred with each generation, allowing recessive traits that require inheriting a copy of the gene from both parents to become more common. For example, lumbosacral transitional vertebrae (LSTV), a recessive deformity of the spine that likely damages nerves controlling tails and hind legs, is normally seen in 1% of wolves but on Isle Royale, 33% have it. Such a deformity inhibits a wolf’s ability to hunt, making it difficult to get food necessary for survival.
While the level of inbreeding has increased over the years, introduction of a new set of genes with the arrival of an immigrant wolf rescued it and helped the population grow for a time. This wolf, nicknamed the Old Grey Guy, crossed another ice bridge to the island in 1997, and following his arrival, the population size rose again. The inbreeding coefficient, an indication of genetic diversity in the population measured from zero (non-relatives) to one (complete relatives), peaked around 2000 at 0.8 before falling to 0.1 just a few years later as the pups that the Old Grey Guy sired became a part of the adult population. This coefficient is on the rise yet again, reaching 0.3 in 2010 as his descendants become more prominent in the population. At the same time, the population size peaked at 30 in 2006 before dropping to nine wolves in 2012, the lowest observed number on the island in the 55-year study.
As the single remaining member of the Middle Pack, a specific wolf family on the island, Isabelle’s female assailant is likely the most genetically diverse female on Isle Royale. Such genetic diversity is necessary to produce offspring that do not have harmful recessive traits and so are capable of surviving. So, while Isabelle fights for her life, her assailant fights for the prolonged survival of wolves on the island. Nonetheless, the Old Grey Guy’s introduction of new genes shows that inbreeding is inevitable in the isolated population. The female assailant may be able to produce viable offspring for now, but the issue remains of the imminent decline of genetic diversity in future generations. This inbreeding will lead to a higher occurrence of harmful traits that will threaten the survival of the entire wolf population on the island.
After observing the population for 55 years, it is natural to care about the wolves and hope that they will continue to survive on the island. With the inevitable threat of dying out, it is tempting to seek ways to aid the population – in vitro fertilization, introducing new wolves, anything that can be done in desperation to bring genetic diversity to the island population to help them thrive. But this contradicts the belief that nature is meant to run its course without human intervention. John Vucetich, the lead researcher on Isle Royale, acknowledges this dilemma stating, “We have so much to learn about how we can relate to nature.”
When I synthesize my standard molecule in a reaction consisting of a drug, guanine, and cysteine for biological analysis in my lab, I see it not just as organic chemistry but also as a reaction in the body. It is a simplified biological system. The cysteine is part of a large protein and the DNA is part of an even larger chromosome. The drug has already been infused into the blood stream, distributed throughout the body while associating and dissociating with various biomolecules, absorbed into the cells, and has now entered the nucleus of a cancer cell. When the reaction occurs inside the cell as it is occurring on my lab bench, it will create a lesion to the DNA so bulky that it could stop DNA replication requiring either repair or apoptosis of the cell (ideally) thus killing the cancer cell.
It is so much more than understanding organic chemistry and performing a chemical reaction. It is looking at a specific part of that drug’s effect on the body and seeking to understand it on a molecular level. Yes, the drug is effective at treating certain cancers, but it is also useful to know why the drug is so capable. If we look to further understanding the chemical interactions that occur, perhaps we can be able to design future generation drugs from this drug to improve the efficacy and specificity of treatment to better eradicate cancer.
But we wouldn’t understand it if we didn’t have chemistry.














{kind=link}